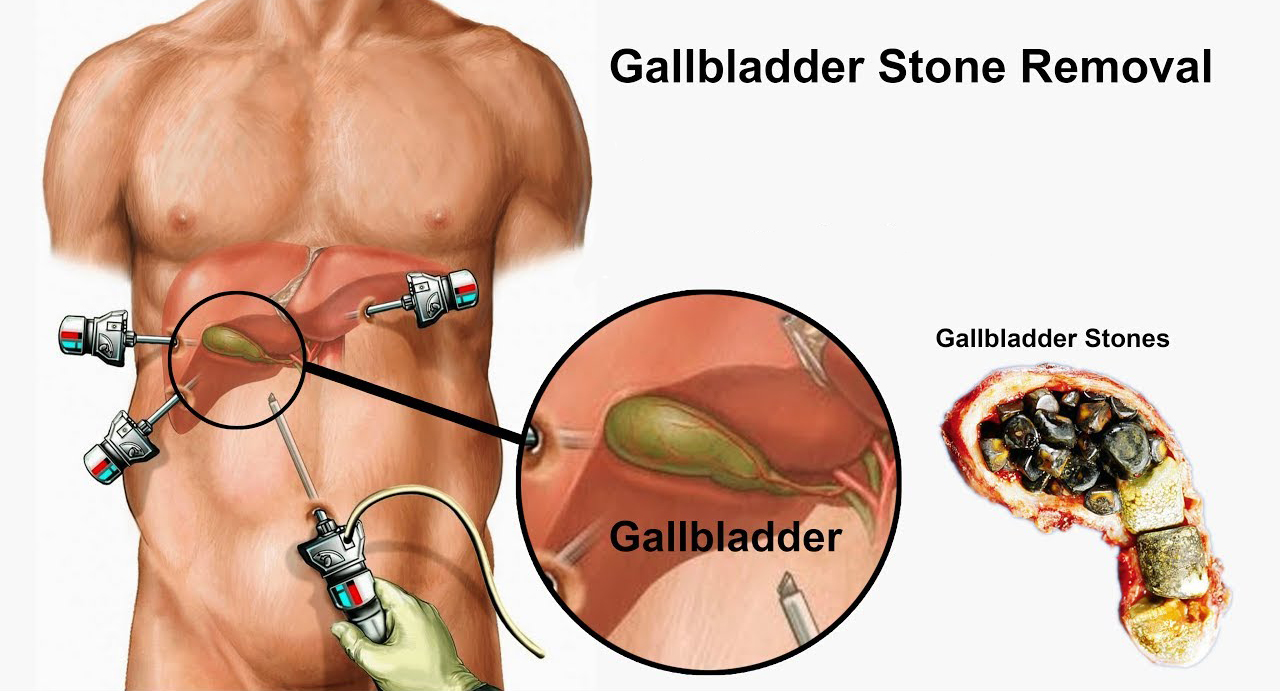
Laparoscopic Cholecystectomy is one of the commonest general surgical procedures performed worldwide. It involves removal of Gall bladder by making tiny holes (5-10mm) in abdomen and using laparoscopic instruments .This surgery is done under general anaesthesia.
THE GALL BLADDER
Gall bladder is a small distensible sac which lies underneath the Liver and has a storage capacity of 50-100 ml. Its main function is to store secretions from the liver (Bile juice) and release it following food intake, thus aiding in digestion. The sac has only one opening which acts as both inlet and outlet.
WHY DO GALL STONES OCCUR?
There are several theories to it and usually combinations of factors contribute. Increased amount of cholesterol in bile as seen in obese individuals, haemolytic conditions resulting in high bilirubin levels, subclinical infections and decreased contractility of gall bladder thus resulting in stagnation, all may contribute to gall bladder stone formation.
WHO SHOULD UNDERGO SURGERY?
The overall prevalence of gall bladder stones is high (about 1- 3 in 100 persons screened) and healthy asymptomatic patients do not need any form of treatment. The occurrence of complication is usually preceded by symptoms and once the patients are symptomatic, they are advised to undergo surgery in order to relieve pain and prevent complications.
WHAT ARE THE SYMPTOMS CAUSED BY GALL STONES?
Most common symptom is that of pain. It is usually sudden onset rapidly intensifying pain in right upper abdomen or sometimes in the center of abdomen lasting for 1-2 hours or more. Pain may be associated with nausea, vomiting or right back/shoulder pain. Pain is usually triggered by a fatty meal. When complications occur patients may have more severe and long lasting pain, pain radiating to the back, fever, jaundice etc.
ARE THERE ANY OTHER ALTERNATIVES TO SURGERY?
No, currently the only effective treatment for symptomatic Gall stone disease is complete removal of the Gall bladder. Just removal of stones is not useful as it is mostly a malfunctioning gall bladder and the stones will recur soon. Trial of medical management to dissolve gall stones have not shown to be of any benefit till today’s date.
ON THE DAY OF SURGERY
Patients for elective laparoscopic cholecystectomy are usually admitted in the morning of the day of surgery. Patients are advised overnight fasting, whole body bath with antiseptic soap and removal of ornaments, nail polish etc. All routine medications need to be continued unless specifically advised not to by the physician .The surgery will be performed under General Anaesthesia.
DURATION OF SURGERY
Varies between 45 minutes to 2 hours or more depending on the complexity in individual patient
THE SURGERY
Laparoscopic Cholecystectomy is performed by standard 4 port technique which generally involves one cm incision at the umbilicus and three 5mm incisions in upper and right side of abdomen. In the operation theatre patient may have naso-gastric tube and urinary catheters inserted which are generally removed on table or immediate post operatively.
IMMEDIATE POST OPERATIVE PERIOD
Pain: Though laparoscopic surgery is associated with significantly less pain compared to open surgery , the pain thresholds vary between individuals . Patients are initially given IV pain medications which is then switched over to oral tablets. Some patients may develop right shoulder pain due to diaphragmatic irritation caused by gas inflated into the abdomen during surgery which subsides in a day. In most patients post operative pain reduces in two to three days but wound site pain may continue up to 2-3 weeks time. Patients may have some soreness in throat for 1-2 days secondary to endotracheal intubation for anaesthesia.
Nausea and Vomiting: It is a fairly common symptom during early post operative period lasting for about a day and can be reduced with medications
Post operative Fatigue: This usually improves with time. Surgical stress, anaesthetic and analgesic drugs used, sleep deprivation are all contributory factors
DVT Prophylaxis: It involves combination of measures like elastic stockings, subcutaneous heparin injections, oral anticoagulants, physiotherapy and early mobilization from bed during post operative period depending on the risk profile of the patient.
Drain care: A drainage tube may be placed into right side of abdomen in selected patients, which is removed in the ward or OPD during post operative period. Care needs to be ensured to prevent tube dislodgement
Diet: Following uneventful laparoscopic cholecystectomy patients can usually resume oral diet in 4-6 hours following surgery. Patients are advised to have light meal as tolerated on the night of surgery.
Discharge from Hospital: Patient may be discharged on the day of surgery or the next day depending on patient comfort and feasibility of home care.
POST OPERATIVE FOLLOW UP
Wound care: Wound dressings may be removed on 2nd day following surgery. Patients are advised to take normal bath and maintain wound hygiene. Any excessive pain, redness or discharge from surgical wounds needs to be reported.
Sutrure(Stitch) Removal : Depending on the type of suture material used it can be left to get self absorbed or needs to be removed between post operative day 8-10.
Biopsy report: Gall bladder after removal is sent for routine histopathological examination and will be communicated during OPD visit.
RETURN TO ROUTINE ACTIVITY AND WORK
The average time taken to resume work is about 10-15 days. Normal household work may be started much earlier depending on individual patients. Most patients are mostly pain free in about a week after surgery
WHAT ARE THE INTRAOPERATIVE AND EARLY COMPLICATIONS OF LAPAROSCOPIC CHOLECYSTECTOMY?
No Operation is completely risk free. During Laparoscopic Cholecystectectomy there is a minimal but realistic chance of intra operative, early or late post operative complication.
Intra operatively there may be excessive bleeding, Injury to bile ducts or other viscera, injury to major blood vessel supplying the Liver, some of which may require converting to an open operation.
During Immediate post operative period there may be Cardio-Pulmonary complications, DVT and related complications, Bile leak leading to biloma or peritonitis , slippage of gall bladder stone into bile duct causing Jaundice and rarely pancreatitis . Small percentage of patients may develop surgical site wound infection
LATE POST OPERATIVE AND LONG TERM COMPLICATIONS OF LAPAROSCOPIC CHOLECYSTECTOMY
Persistent symptoms: A small but significant percentage of patients may continue to have symptoms even after surgery. There are several causes, some of which include missed CBD stone, sphincter of oddi (SOD) dysfunction and co existing problems like acid peptic disease, irritable bowel syndrome(IBS) or neurologic disorders .
Post cholecystectomy diarrhoea: About 10 percent of patients report diarrhoea following cholecystectomy . This is mainly attributed to bile salts induced laxative effect on colon. This is self limiting in majority of patients and only a small percentage of patients may require medications in the form of anti diarrhoeal or bile acid sequestrates (cholestyramine). Patients are advised to maintain hydration, increase fibre intake and avoid lactose based foods.
Post Cholecystectomy biliary strictures: These are very rare complications and may manifest as pain ,jaundice , itching and fever several weeks to months following cholecystectomy. Most of these patients would have had bile leak during early post operative period.
Port site hernia: Persistent pain or bulge at operative site near the umbilicus may indicate hernia formation. Obesity, history of surgical site infection, constipation, and persistent cough increases the risk of hernia.
Port site Sinus: In cases where there was intra operative spillage of stones, patients may develop discharging sinuses at drain or port sites. This would warrant wound exploration. Rarely this may be caused due to atypical mycobacterium infection
A better life starts with better health



